Are site referrals truly higher quality than advertising leads?

This is just one myth we busted!
Download the full eBook to explore all the data and discover what’s really driving quality in patient recruitment.
Why sites were seen as the superior patient recruitment
In clinical research, long-held beliefs about patient recruitment have shaped how trials are designed and executed. One of the most persistent assumptions is that patients referred by clinical sites are inherently higher quality, more engaged, more likely to qualify, and more likely to remain in the study than those recruited through digital channels.
At first glance, this belief makes sense. Site staff have personal relationships with their patients, access to their medical records, and the ability to discuss participation in detail. These human interactions seem to offer a layer of trust and precision that mass digital outreach could never match.

The evolution of data-driven patient recruitment
However, recent data tells a different story. When recruitment outcomes are analyzed objectively, digital recruitment often performs just as well, if not better, than traditional site referrals.
Digital strategies can now leverage advanced targeting, pre-screening tools, and personalized engagement workflows that rival the precision of site-based referrals. Instead of being broad and impersonal, digital outreach has evolved into a data-driven, patient-centric approach capable of identifying high-quality participants who might never be reached otherwise.

The myth of superior site-sourced patient recruitment
At the heart of this myth is a simple assumption: proximity equals quality. Patients from a site’s own database are often seen as a safer bet because they already have a relationship with that provider, and site staff know their medical histories and conditions.
This traditional approach feels familiar and dependable. But it can also overlook the limits of relying only on a site’s existing patient pool and underestimate how precise and effective modern digital recruitment has become.
Today’s digital strategies can identify, pre-screen, and educate potential participants in ways that enhance, not replace, traditional site recruitment.
That extra expertise can help you prioritize leads more quickly for a reduced costs. Marketing Sherpa estimated that 79% of all leads never convert, emphasizing a need for someone with experience in lead scoring so that you’re not chasing down bad leads. Sopro found that with the same number of leads coming in, better follow-up and strategy can make them about 50% more likely to turn into qualified prospects at 33% lower cost.
But does this apply to patient recruitment in clinical trials?
A 2025 study in JMIR Mental Health examined how digital tools are reshaping patient recruitment for clinical trials involving depressive symptoms. Analyzing over 500 participants, researchers found that agencies using digital tracking and social media targeting cut their cost per qualified lead by 83% from about $107 to just $18. These methods didn’t just lower costs; they accelerated timelines and expanded reach, often outperforming traditional site-based referrals.
In addition, a systematic review published in Journal of Medical Internet Research found that online recruitment methods significantly outpaced traditional clinic/site-based approaches: across 61 studies, the incidence rate ratio (IRR) for online vs offline recruitment during active days of recruitment was 4.17, meaning digital strategies brought in participants more than four times faster than offline methods.
Download Now: Patient Recruitment Myth Busters

Myths don’t move clinical research forward. Data does.
We’re setting the record straight on the biggest misconceptions in patient recruitment. See the full list of myths we’ve debunked by clicking below!
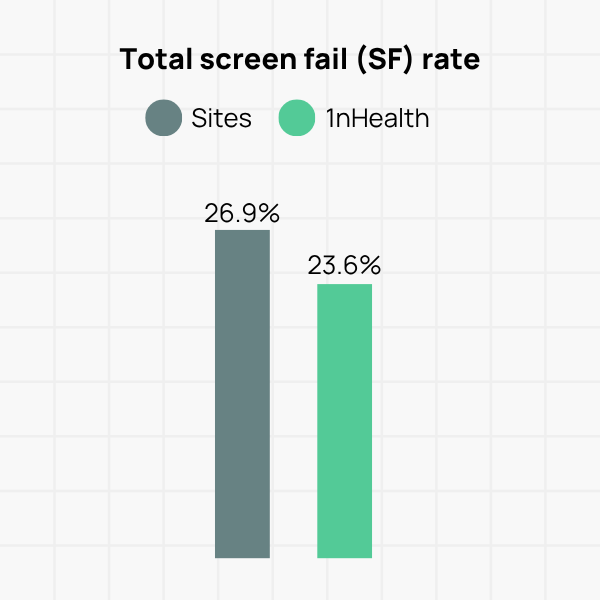
Case Study: Site referrals 14% more likely to screen fail in gastrointestinal study
In a recent gastrointestinal study, 1nHealth supplemented site-based recruitment. After five months, digital referrals had a 23.6% screen fail rate versus 26.9% for site-sourced patients.
The difference, while seemingly small at 3.3 percentage points, is statistically significant when you consider the recruitment scale of a large trial taking in thousands of submissions.
This isn’t meant to be a critique of the hard work that site teams do. Their role is absolutely critical. This should encourage us to rethink traditional assumptions about patient quality and may allow site staff to focus on what they do best: guiding patients personally through the enrollment process.
How does digital patient recruitment deliver quality patient referrals?
Seeing these numbers, the immediate question is: why? How can a digital approach, which seems so removed from the patient, produce more qualified referrals? The answer lies in the precision, scalability, and data-driven nature of the process. It’s not about reaching everyone, it’s about targeting the right patients more efficiently.
Precision targeting at scale
Traditional methods are limited by the size and scope of a site’s patient database, but personalization is necessary for patient recruitment. Cropink found that 80% of consumers were more likely to engage with a brand when there was at least a “moderate level” of personalization to it.
Digital recruitment breaks through those walls, reaching potential participants far beyond a clinic’s geographic or demographic bubble.
Using sophisticated algorithms and platform tools, we can target individuals based on:
- Interests and Behaviors: People actively searching for information about their condition.
- Demographics: Age, location, and other criteria relevant to a study’s protocol.
- Lookalike Audiences: Finding new people who share characteristics with patients who have successfully enrolled in past trials.
A rigorous, multi-step vetting process
A 2023 study of 25 general practice sites recruiting for an RCT found that clinical staff spent an average of 3.7 hours in recruitment effort per patient randomized. With that number reduced by even 10% through stronger pre-referral vetting, that’s an average of nearly 30 minutes saved per randomization.
One of the biggest advantages of digital recruitment is how it helps site teams focus on what matters most: qualified, ready-to-engage patients.
Rather than passing along every name that clicks an ad, the process is designed to ensure only the strongest matches reach the site.
It starts with a carefully crafted pre-screener built around each study’s inclusion and exclusion criteria. This step filters out anyone who isn’t a good fit, keeping the process aligned with the protocol and saving valuable site time.
By the time a referral lands in a coordinator’s inbox, it’s already been through multiple layers of qualification, so staff can spend their time with participants who are most likely to enroll.
Data-driven optimization
One of the biggest strengths of digital recruitment is its ability to learn and adapt in real time. Every click, every pre-screener submission, and every piece of feedback from a site becomes a data point we can act on.
We use that data to continuously fine-tune our approach. If certain ads perform better, we shift more budget their way. If a pre-screener question causes too many people to drop off, we revisit the wording or placement. And if one channel’s referrals aren’t converting as well, we adjust the targeting to improve quality.
Direct-to-patient recruitment isn’t a static process, it’s a system that gets smarter with every interaction.
Rethinking patient recruitment for your next clinical trial
The idea that site-sourced patients are always higher quality is outdated. A well-run digital recruitment strategy can not only match that quality but, in many cases, surpass it.
For sponsors and CROs, these findings are a prompt to take a fresh look at recruitment strategies and budget priorities. Holding on to an old assumption could mean overlooking one of the most effective tools available. It can also lead to slower enrollment, heavier site workloads, and higher costs.
Our goal in sharing this is simple: to encourage a more data-driven, evidence-based approach to patient recruitment. It’s time to move past outdated beliefs and focus on what truly helps bring new therapies to patients faster.

Explore more patient recruitment myths debunked
Myth #1
Site referrals are higher quality than advertising leads
Myth #2
You have to look clinical to be seen as credible
Myth #3
We can’t use TikTok to recruit patients

Myth #4
You can’t predict recruitment performance accurately

Myth #5
Databases are the most reliable patient sources