The gap is not a question of awareness. People know depression exists. The distance sits between recognizing it and reaching the care that could help.
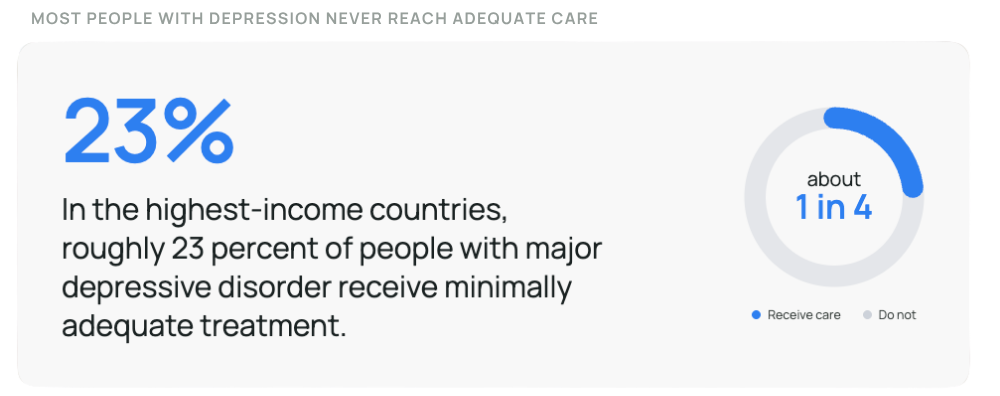
Most people with depression never reach adequate care
The pattern holds globally. A 2022 systematic review and meta regression in PLOS Medicine examined treatment coverage for major depressive disorder across 84 countries. Even in the wealthiest settings, only about
23 percent of people with MDD received minimally adequate treatment.
²
In major depressive disorder, the illness itself works against the action enrollment depends on. The thing we ask someone to do; reach out and raise a hand, is the thing their condition is actively suppressing.
For a person living with depression, that figure has a texture. It is the appointment never booked. The form opened and closed. The intention that never survived contact with a hard morning.
The screener is its own hurdle
By the time someone reaches a screener for an MDD trial, they have usually tried more than the form will ever ask about. Therapy that helped for a while. Medications that worked, until they stopped, or worked at the cost of feeling like themselves. So completing that screener is not a small administrative step. It is a decision made against the pull of the illness, on a day the illness was arguing against it.
This is where recruitment either helps or quietly fails. The variable is not whether a person is motivated. It is whether outreach meets them where the condition has left them. Messaging that demands energy a person in a depressive episode does not have will lose them. Messaging that lowers the cost of the first step will not.
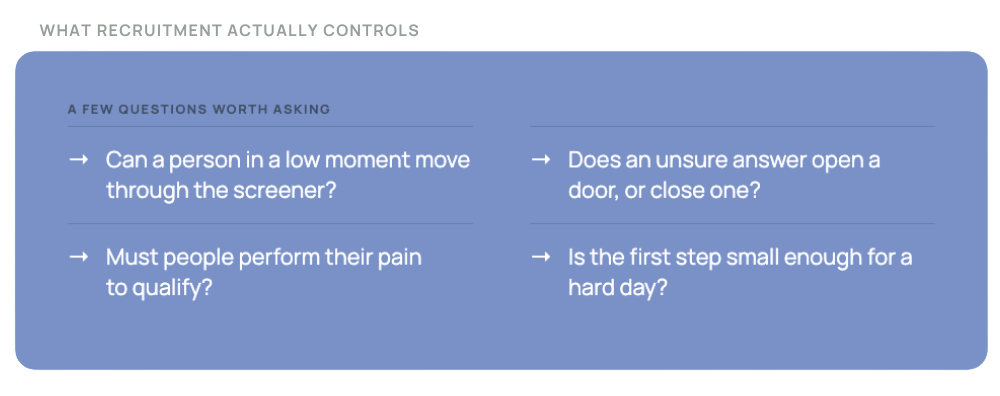
What recruitment actually controls
Recruitment cannot change a diagnosis or rewrite eligibility criteria. What it can control is whether the first contact a person has with a study makes the next step feel possible.
A few questions worth asking of any depression trial recruitment effort:
If those answers are unclear, an enrollment gap is being built in before a single person reaches a site.
The form looks small. The decision behind it is not.
Every screener submission for a depression study represents a person who, on a day their condition told them not to bother, decided to try anyway. Recruitment that respects what that costs is not only kinder. It is how these studies fill.
At 1nHealth, we build recruitment for mental health research around that reality. We write in plain language, we treat an uncertain answer as the start of a conversation, and we design the first step to be one a person can take on their hardest day.